I admit I was horrified when I read this press release. My first thought was what will these people
think of next. Nothing about diabetes can be this cut and dried.
When I arrived at the image of the hand that the topics assigned to
each part, I really was at a loss for understanding.
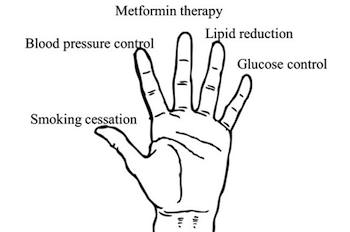
This image shows the "lend a hand" illustration: an open palm facing out. The five major forms of diabetes interventions are arranged in descending order of importance from thumb to pinky. The order is smoking cessation, blood pressure control, metformin therapy, lipid reduction, and glucose control, respectively.
Image credit: Modified by Heather White, Tufts University
To accomplish each in the order as
described, what are they going to do when they have a patient that
has never smoked a cigarette? Will they have to have the patient
learn to smoke just to have the patient cease smoking? What will
they do for the patient that does not have hypertension? Are they
going to insist that a person take metformin when the person may be
able to manage diabetes with nutrition and exercise? Are they going
to force people with normal lipid panels to take statins? Then we
arrive at what they consider the least important intervention –
glycemic management.
Now granted, the majority of people
newly diagnosed with type 2 diabetes will have some of the
requirements needing intervention, but why would they not do all at
once. I would have hated for them to have done one at a time on me.
This does seem to be the recommendation that they suggesting –
treating each in the order they have identified until it is under
management and then moving to the next digit of the hand. This has
me wondering about the conflicts of interest and how much influence
this has on their decision.
The senior author lamely admits, "Some
degree of glycemic control is necessary to prevent symptoms."
"It's just that the return on investment is low when we try to
push patients with diabetes to get their blood glucose as close as
possible to normal."
It seems to me that the authors are too
tied up with return on investment to care about the overall health of
the patient. To these authors, I would remind them that health care
is not this cut and dried and not every patient will present with the
same needs. Yet they seem to be of the opinion that every patient
should be treated the same and left no room for adapting their model
to fit the patient. Until the medical community stops practicing a
“one-size-fits-all” regimen, we as patients need to stay alert to
be sure we receive the treatment we need and the explanation of why
we need the treatment.
You should read another interpretation
of this by Tom Ross when he discusses also using the other hand. I
found his blog very interesting.
No comments:
Post a Comment